
Moving Outcomes with Ambulation
![]() Print this Article | Send to Colleague
Print this Article | Send to Colleague
The Centers for Medicare and Medicaid (CMS) determined that all inpatient falls are preventable and therefore, substantial reimbursement funds have been withheld (CMS, 2006). The Centers for Disease Control (CDC) estimate that inpatient falls occur as frequently as every 11 seconds and thirty percent of those falls result in injuries that are expected to cost approximately 54.9 billion by 2020 (CDC, 2013). Falls are reported publicly as a measurement of quality and hospitals have issued a multitude of safety initiatives to prevent falls. Gowden, Shorr, & Inouya (2017) recognized that as organizations have implemented programs intended to prevent falls, patients have been experiencing functional decline, or loss of mobility because of their staying in bed for up to 95% of their hospital stay (Brown, Redden, Flood, & Allman, 2009). Multiple studies have shown correlations between mobility and positive outcomes and nurses admit that ambulation is the most frequent missed care event (Kalisch, Tschannen, & Lee, 2012) due to the fear of a patient falling, lack of staff and/or assistive devices (Doherty-King & Bowers, 2011). The nursing staff have conflicting priorities with physicians writing activity orders that, if carried out, place the patient and nurses at potential risk to violate the mandates from hospital administration to maintain safety. Another conflicting priority comes from the patient, who must always be satisfied and would often prefer to stay comfortably in bed as opposed to working through the necessary pain that often accompanies healing
Mobilizing patients requires overcoming the obstacles of equipment management, staff distribution, patient expectations, and safe patient handling. Growdon, Shorr, & Inouya, (2017) reveal that recent studies on fall interventions do not support a decline in falls or falls with injuries, however; there has been a significant rise in immobility (Waters, et al., 2015). Immobility can lead to functional decline in as little as 48 hours for a hospitalized patient and the loss of 5% of muscle mass in 24 hours (King, Yoon, Pecanac, Brown & Mahoney, 2014). An independent geriatric patient can arrive to the hospital for an elective procedure, stay for an average length of stay of 3.6 days for the routine surgery, and if the patient remained in bed 95% percent of the time, they could experience functional decline and subsequently be admitted to a rehab or other skilled nursing facility. Ambulation is the activity of daily living most often lost during functional decline and for geriatric patients, ambulation represents independence. Although well-established through multiple studies to be beneficial for patients, mobility and ambulation remain underutilized in the acute inpatient setting. Geriatric patients (over age 65) are at the highest risk and the mobility programs can help maintain independence post hospitalization (Brown, et al, 2016).
With no clear reduction in falls, despite the CMS mandate for the never event, and a rise in poor outcomes such a post-acute care needs, nurse leaders should examine the focus of care and consider ambulation as a strategy with a high return on investment. One unintentional positive finding from a mobility study was a reduction in falls (Brown, et al, 2016). Other positive interventions being utilized that might be useful for nurse leaders include medication monitoring for delirium, utilizing sitters as part of mobility teams, restructuring equipment for efficiency to assist in mobility. Gowden, Shorr, & Inouya (2017) recommend replacing fall prevention teams with mobility teams and alarms with mobility trackers to truly move patient outcomes with ambulation.
References
Brown, C.J., Foley, K.T., Lowman, J.D. Jr, et al. (2016). Comparison of post hospitalization function and community mobility in hospital mobility program and usual care patients: a randomized clinical trial. JAMA Intern Med. 176(7):921-927.
Brown, C.J., Redden, D.T., Flood, K.L., & Allman, R.M. (2009). The under-recognized epidemic of low mobility during hospitalization of older adults. Journal American Geriatric Society, 57(9), p. 1660-1665.
Centers for Disease Control and Prevention (CDC). (2013). Cost of falls among older adults. Retrieved from http://www.cdc.gov/homeandrecreationalsafety/falls/fallcost.html
Centers for Medicare & Medicaid Services (CMS). (2006). Eliminating serious, preventable and costly medical errors – never events. Retrieved from http://www.cms.hhs.gov/apps/media/press/release.asp?=1863.
Davidson, S., Weberg, D., Porter-O’Grady, T. & Malloch, K. (2017). Leadership for evidence-based innovation in nursing and health professions. Burlington, MA: Jones & Bartlett Learning.
Doherty-King, B., Bowers, B. (2011). How nurses decide to ambulate hospitalized older adults: Development of a conceptual model. Gerontologist, 51(6), p. 786-797.
Growdon, M.E., Shorr, R.I., & Inouya, S.K. (2017). The tension between promoting mobility and preventing falls in the hospital. JAMA Internal Medicine, 177(6), p. 759-760. doi:10.1001/jamainternalmed.2017.0840.
Kalisch, B.J., Tschannen, D., Lee, K.H. (2012). Missed nursing care, staffing and patient falls. Nursing Care Quality, 27(1), p. 6–12.
Waters, T.M., Daniels, M.,J., Bazzoli, G.J., et al. (2015). Effect of medicare’s nonpayment for hospital-acquired conditions: lessons for future policy. JAMA Intern Med. 175(3):347-354.
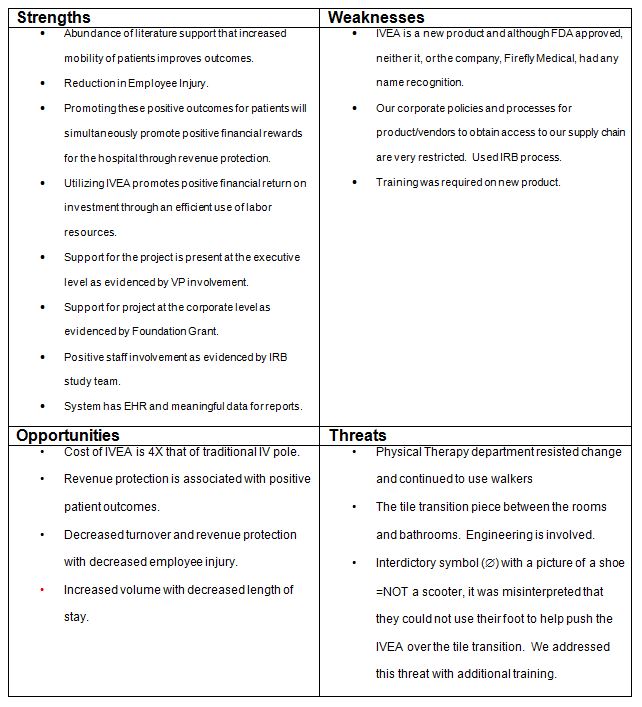
Appendix A
SWOT Analysis Table
![]()
![]()
![]()
![]()
